What if we’ve been telling the wrong story about rural healthcare?
Hi Neighbor,
For a lot of folks, programs like Medicaid and Medicare get framed as personal support. And they are. But in rural communities, they also hold together the places people rely on every day. The clinic that can keep its doors open. The hospital that can afford to keep offering maternity services. The provider who can stay in town instead of leaving. These programs don’t just cover care, they keep care available.
Programs like Medicaid, Medicare, and Affordable Care Act coverage can go by different names depending on the state or policy, but in rural communities, their impact shows up in similar ways: not just in individual lives, but in whether entire health systems can keep going. In places already facing hospital closures and long drives for care, that difference is everything.
That picture starts to come into focus when you listen to people living it.

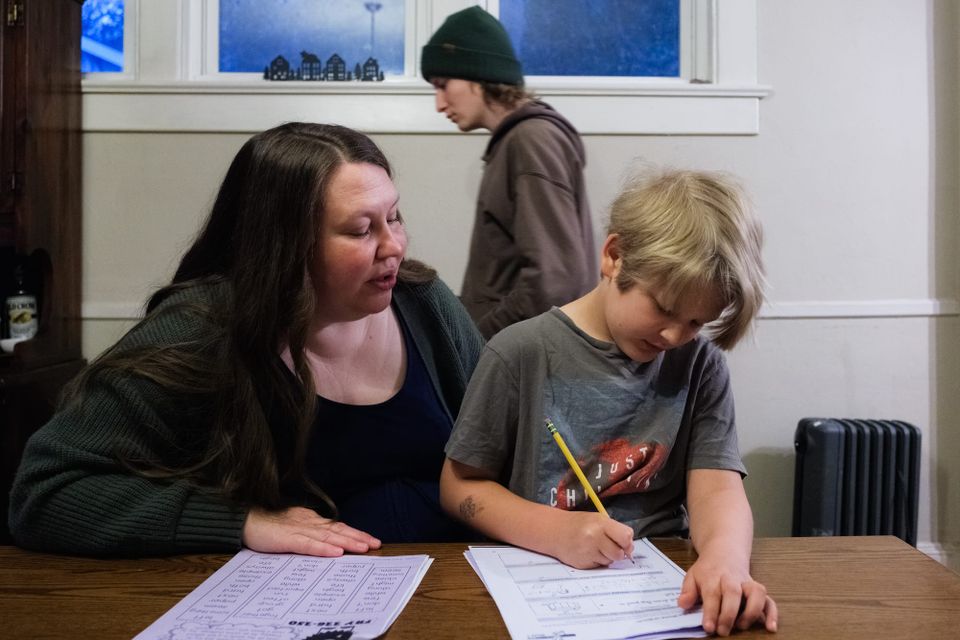
In North Carolina, Shanna Peele has spent 15 years teaching, raising her family, and showing up for her students. For much of that time, Medicaid was what made that work possible: covering her pregnancies, her children’s care, and health needs allowed her to stay in the classroom. “It’s that security in knowing that at least something’s going to be OK,” she said. “At least I’m going to be somewhat healthy. My baby is going to be healthy and taken care of.”
That stability didn’t stop at her front door. It showed up in her school; in therapists, in services, in a classroom that could keep running because both teachers and students had what they needed.
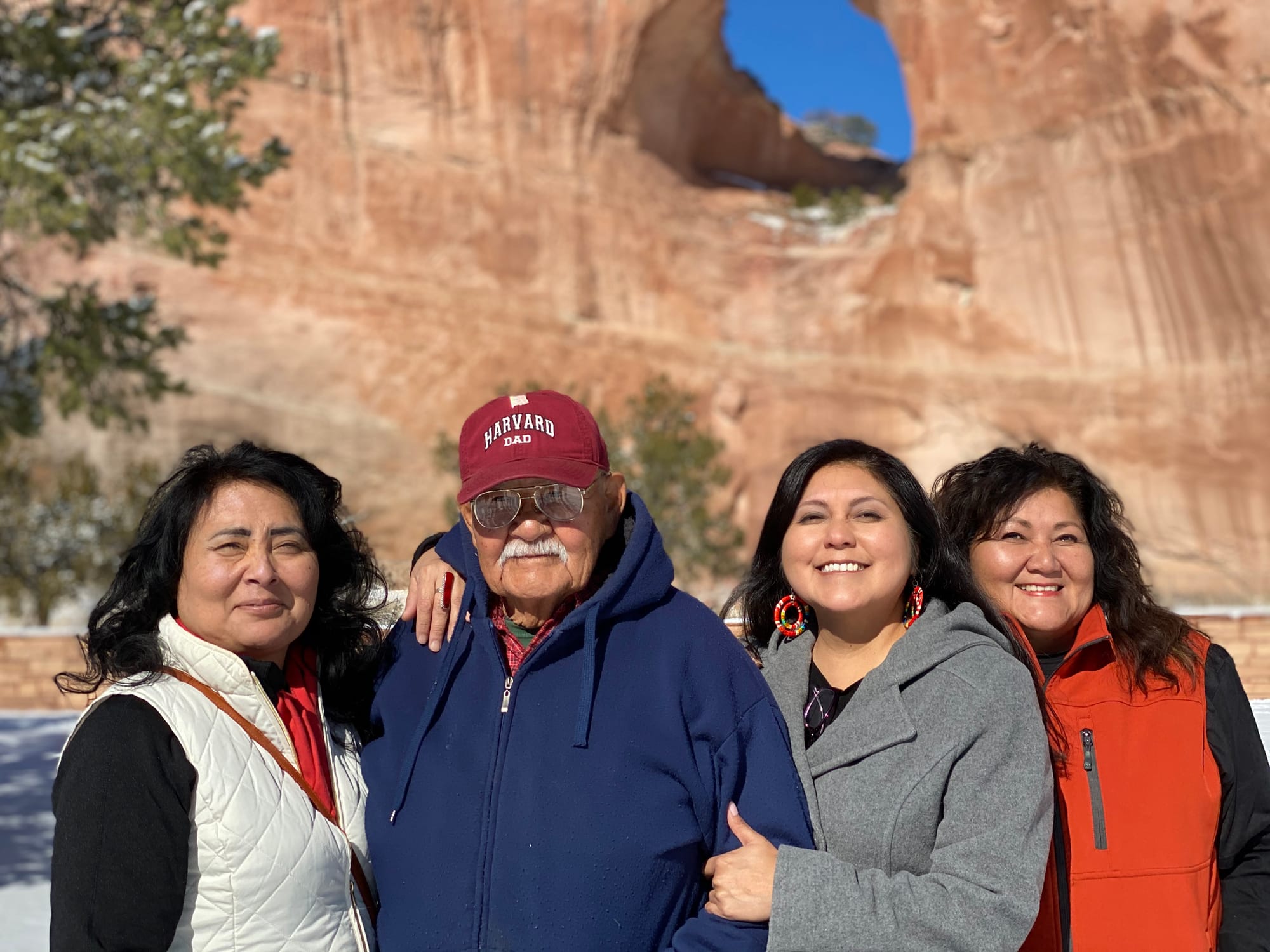
In Kayenta, Arizona, James Parrish has spent his life in service: to his country, his community, and his neighbors. But in a place where specialized treatment can mean driving hundreds of miles, access to care isn’t guaranteed. Through a mobile Veterans Affairs clinic and services connected to Indian Health Services, Parrish received life-saving care that keeps him going today — driving neighbors to appointments, speaking to students, and staying active in the community that depends on him.

Meanwhile, back in western North Carolina, Russell Layson spent his days driving winding back roads to deliver food through the Healthy Opportunities Pilot, a Medicaid program designed to improve health by addressing everyday needs like food, housing, and transportation. But what he saw wasn’t just full refrigerators. He saw homes stabilizing, people making it to appointments, and neighbors starting to feel better, physically and mentally. “I started noticing the houses were getting cleaned up more, and I started seeing the positives in their mentality,” he said.
That kind of support didn’t just improve individual health. It reduced healthcare costs, supported local jobs, and helped people stay connected to their communities. And when the program was cut, those gains didn’t just disappear for one person, they were felt across the entire system, from families to providers to the local economy.

Across these stories, a pattern starts to emerge.
In rural communities, care doesn’t exist in isolation. It’s built and sustained by people. Neighbors delivering food, teachers holding classrooms together, providers finding ways to reach patients miles down the road. Programs like Medicaid and Medicare don’t replace that work. They make it possible. And when they work, the effects travel through clinics, schools, small businesses, and the everyday systems people depend on.
So if we’ve been telling the wrong story about these programs, it’s because we’ve been telling it too small. We’ve been talking about individuals, when the reality is much bigger – about whether care exists at all, and whether communities can keep going.
The people in this newsletter know that story well. They’re the ones doing the work every day to keep their communities healthy and connected. They see what’s working. They see what’s at risk. And they’re the ones carrying these stories forward.
In gratitude,
Resource Rural